
As approaches to ageing change, should we change our approach to diseases of ageing?
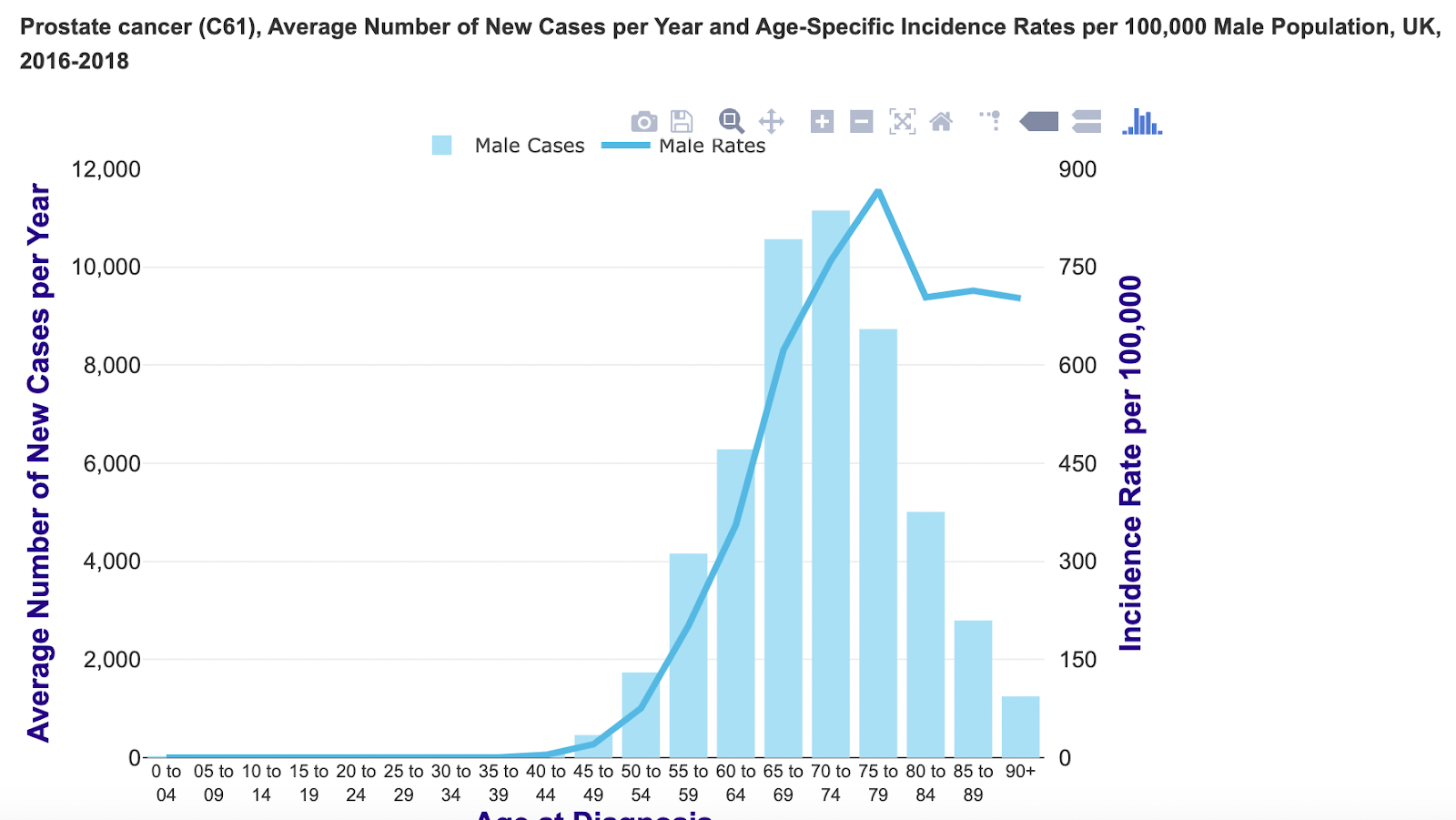
As a clinic we specialise in treating men with prostate cancer – a disease of ageing Nearly 60% of all prostate cancers are diagnosed in men over the age of 65. The actual age distribution looks like this, as presented by Cancer Research UK
That prostate cancer is a disease of ageing is well understood and rarely disputed. What is less understood is how increased longevity in many population groups is shifting our attitudes and approaches to ageing and by extension, our approach to treating diseases of ageing.
For some, an increased ageing population means a drain on scarce healthcare resources. For others it signals a renewed emphasis on maintaining quality of life.
This was brought into perspective in recent reporting on cancer outcomes in the UK, which showed how people successfully treated for cancer are living longer lives with side effects from their treatment, often impairing their quality of life.
It argued that “for decades, doctors have been so focused on defeating the cancer that they have often overlooked what comes next. And the side-effects of many of these treatments — particularly the older forms of chemotherapy, radiotherapy and surgery — can be brutal.”
As one commentator pointed out,
“it does become an issue that as people survive longer and longer, they are living longer with the side-effects of the treatments. Quite rightly, research funders and clinicians have been focused on tackling the cancer, but there has been a lot less attention paid to the side- effects.”
And the report pointed to innovations that have taken place to pave the way for “kinder” cancer treatments. According to Michelle Mitchell, chief executive of Cancer Research UK:
“Kinder treatments can have immediate impact in the short term — allowing people to complete their treatment without interruption — and they also reduce the risk of long-term complications, improving the continuing health of people who have had cancer so that they can lead better and healthier lives.”
This is a welcome approach to treating cancer in older patients and reflects the converging forces of discovery and dissemination of new therapeutic approaches to cancer which are providing expanded treatment choices and demographic trends that are driving increases in population life expectancy. It also reflects a growing level of patient advocacy and patients’ desire to maintain quality of life as they age.
Another way that changing views on ageing are impacting how we treat men with prostate cancer is the emerging acceptance and application of biological age v chronological age in managing patient care.
A group of researchers in the USA are developing a framework based on biological age to improve the care of individuals with adult cancers:
“The practice of oncology will involve care of a growing population of individuals with mid- and late-life cancers. Managing these individuals is complex based on differences in biological age at diagnosis. Biological age is a measure of accumulated life course damage to biological systems, loss of reserve and vulnerability to functional deterioration and death. Biological age is important because it affects the ability to manage the rigors of cancer therapy, survivors’ function, and cancer progression. However, biological age is not always clinically apparent.”
They argue that building an understanding of the differences in biological ageing “could ultimately allow clinicians to better personalize treatment and supportive care, develop tailored survivorship care plans, and prescribe preventive or ameliorative therapies and behaviors informed by aging mechanisms.”
We welcome new thinking about ageing as we continually gain insights from our patients and their life experiences. Do you have a perspective on ageing and diseases of ageing? Please join the discussion. We’d love to hear from you.