How Long Can You Live With Prostate Cancer Without Treatment?
Many men diagnosed with prostate cancer — especially early-stage disease — live for years and often die of unrelated causes. Five-year survival for stage 1–2 prostate cancer is almost 100%, and even stage 3 carries around 95% survival. Prognosis depends on stage, Gleason score, age, and overall health, making an individual assessment with a urologist essential.
At a Glance
Many men diagnosed with prostate cancer — especially early-stage disease — live for years and often die of unrelated causes. Five-year survival for stage 1–2 prostate cancer is almost 100%, and even stage 3 carries around 95% survival. Prognosis depends on stage, Gleason grade, age, and overall health, making an individual assessment with a urologist essential.
Stage matters most – localised prostate cancer (stages 1–2) has near-100% five-year survival; stage 4 drops to around 50%
Not all cancers need immediate treatment – low-risk disease can be safely monitored with active surveillance under specialist guidance
Treatment options are improving – focal therapies like HIFU (NICE IPG756) and NanoKnife- IRE (NICE HTG688) target the tumour while preserving quality of life
Individual assessment is essential – PSA level, Gleason score, MRI findings, and your overall health all shape the right path forward
Understanding What 'Without Treatment' Actually Means
| Active Surveillance | Watchful Waiting | No Management | |
|---|---|---|---|
| Who's it for | Men with low- or favourable intermediate-risk localised cancer who want to delay or avoid treatment | Men — often older or with significant other illness — for whom curative treatment is unlikely to be appropriate | Men who decline all monitoring and intervention |
| Testing | Regular PSA, periodic MRI, and repeat biopsy on a defined schedule | Symptom-led review only; PSA testing if it will guide palliative decisions | No scheduled tests or follow-up |
| Goal | Catch any progression early and switch to curative treatment before the window closes | Maintain quality of life; treat symptoms if and when they arise | None defined — disease follows its natural course unmonitored |
| Outcome | Many men remain on surveillance long-term; ~40–50% convert to treatment within 10 years (ProtecT, Hamdy NEJM 2023) | Disease may progress to symptomatic or metastatic stage; managed with hormone therapy when needed | Risk of undetected progression to advanced or metastatic disease without intervention |
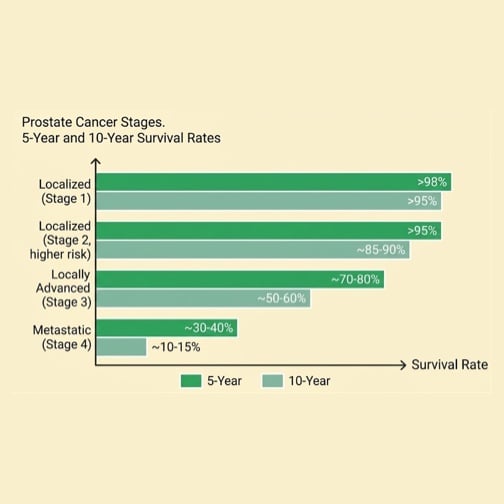
Prostate Cancer Survival Rates by Stage and Risk
| Cancer Stage | 5-yr survival | 10-yr survival | Approach |
|---|---|---|---|
| Stage I – localised | >98% | >95% | Active surveillance; radical prostatectomy; radiotherapy; focal therapy (HIFU / NanoKnife) |
| Stage II – localised (higher risk) | >95% | ~85–90% | Radical prostatectomy; radiotherapy ± hormone therapy; focal therapy for selected cases |
| Stage III – locally advanced | ~70–80% | ~50–60% | Radiotherapy + long-term hormone therapy; radical prostatectomy in selected cases |
| Stage IV – metastatic | ~30–40% | ~10–15% | Hormone therapy (ADT); chemotherapy; novel agents (enzalutamide, abiraterone); palliative care |
What Factors Affect Prognosis?
Prostate cancer risk depends on several factors, some of which cannot be changed. Understanding your risk profile helps you and your GP decide whether prostate cancer screening is appropriate for you.
Gleason score: Lower scores (6-7) typically indicate slower-growing cancer with better outcomes.
PSA levels: Lower PSA levels at diagnosis are generally associated with better prognosis.
Extent of local spread: Whether cancer had reached the seminal vesicles or other nearby structures.
Response to treatment: How effectively the cancer responds to initial therapy.
Overall health: General fitness and any other medical conditions

Is It Ever Safe to Delay Treatment?
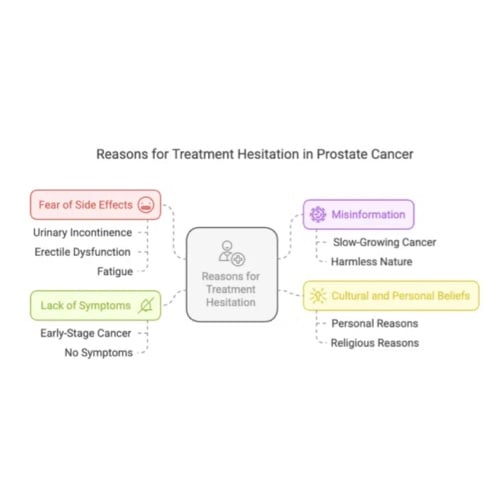
If you've been diagnosed with low-risk prostate cancer, the idea of not treating it immediately can feel deeply counterintuitive — even frightening. That anxiety is completely understandable, and it's one of the most common concerns men bring to their first specialist appointment.
When Should Treatment Be Considered?
A rising PSA trend
A single elevated PSA reading is rarely cause for alarm — levels fluctuate naturally and can be affected by infection, inflammation, or even recent physical activity. What matters is the pattern over time. A consistent upward trajectory, or a rapid doubling in PSA levels, is a signal that warrants closer investigation and a conversation about next steps.
Changes on MRI
Multiparametric MRI (mpMRI) gives clinicians a detailed picture of the prostate at intervals during surveillance. If a previously stable area shows new or increased activity — a lesion growing, or a new area of concern appearing — that change will typically prompt a targeted biopsy to understand what is happening at a tissue level.
A biopsy grade upgrade
Not all prostate cancers behave the same way. If a repeat biopsy shows that cells have become more abnormal — a higher Gleason Score than at diagnosis — that is one of the clearest signals that the cancer is no longer behaving as low-risk, and that curative treatment should be considered promptly.
New or worsening symptoms
The onset of symptoms that weren't present at diagnosis — including new pelvic discomfort, significant changes in urinary function, or unexplained bone pain — always warrants review, even between scheduled appointments.
Could Focal Therapy Be an Option?
For men whose cancer shows signs of progression during surveillance — but remains localised within the prostate — moving straight to radical surgery or whole-gland radiotherapy is not the only path forward. Focal therapy offers a clinically validated middle ground: treating only the area of confirmed cancer, while leaving the rest of the prostate, and the functions it supports, intact.
This matters because the side effects most men fear — urinary incontinence and erectile dysfunction — are largely a consequence of treating the entire gland. When treatment is targeted precisely at the tumour zone, the nerves and tissue responsible for sexual and urinary function have a far greater chance of being preserved. For men who have been monitoring a low- or intermediate-risk cancer, focal therapy can represent the moment when action becomes necessary without the quality-of-life trade-offs of conventional treatment.

A middle path — precision without compromise
Focal therapy treats only the confirmed cancer zone within the prostate, sparing the surrounding healthy tissue that conventional whole-gland treatments cannot protect. For men progressing from surveillance, it is often the step that makes treatment feel possible — without the side-effect profile of surgery or radiotherapy.
Treats only the confirmed cancer area
Preserves surrounding healthy prostate tissue
Significantly fewer side effects than whole-gland treatment
Over 90% of men maintain erections post-treatment (FTC audit, n=265)
NICE-approved (HIFU: IPG756, 2023; NanoKnife/IRE: HTG688, 2023) — available at seven UK locations
Day-case procedure with rapid recovery
HIFU
- Soundwave-based treatment
- Preserves urinary and sexual function
- Day procedure and rapid recovery
Learn More
NanoKnife
- Needle-based treatment
- Preserves urinary and sexual function
- Day procedure and rapid recovery
Learn More
Patient Voices: Choosing the right path forward
Why Choose The Focal Therapy Clinic?
Only clinic using advanced MRI US fusion technologies for precision treatment
Learn MoreWe have helped thousands of people with prostates understand their diagnosis and choose the right treatment for them and their prostate cancer.
Learn MoreWe've assembled a team of urology, radiology, oncology and patient care experts with over 75 years of experience.
Learn MoreOur own data shows that after 1 year of treatment, 90% of clinically significant cancer is eliminated.
Learn MoreQuestions to ask your doctor or nurse

Bring these to your GP appointment, or speak to our team first.
Frequently asked questions

Learn More About Living With Prostate Cancer

Survey of Prostate Cancer Patients Reveals Severe Knowledge Gaps Among Men
How Accurate is a Urine test for Prostate Cancer – and can it replace PSA or MRI?
Is Testosterone Replacement Therapy Safe After Prostate Cancer Treatment?
Any questions?
If you’ve got any questions about your prostate cancer diagnosis or want to know more about HIFU or NanoKnife, don’t hesitate to get in touch with our friendly, knowledgeable team.
Contact the team
Reference List
- Hamdy FC, Donovan JL, Lane JA et al. (ProtecT Study Group). Fifteen-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Localized Prostate Cancer. New England Journal of Medicine. 2023;388:1547-1558. DOI: 10.1056/NEJMoa2214122. Source for the "Did you know" callout on this page — n=1,643 randomised, with cancer-specific mortality of 3.1% in active monitoring vs 2.2% in surgery vs 2.9% in radiotherapy (P = 0.53).
- NICE NG131: Prostate cancer — diagnosis and management. National Institute for Health and Care Excellence, 2019 (updated 2021). nice.org.uk/guidance/ng131
- NICE IPG756: Focal therapy using high-intensity focused ultrasound for localised prostate cancer. NICE, 2023. nice.org.uk/guidance/ipg756. IPG756 supersedes the older HTG667 (2012) HIFU guidance.
- NICE HTG688 (now reissued as HTG688): Irreversible electroporation for treating prostate cancer. NICE, 2023. nice.org.uk/guidance/ipg768. NICE found no major safety concerns short-to-medium term.
- EAU Guidelines on Prostate Cancer, 2024. European Association of Urology. uroweb.org/guidelines/prostate-cancer
- Cancer Research UK. Prostate cancer survival statistics. cancerresearchuk.org — prostate cancer survival
- Office for National Statistics. Cancer survival in England — adults diagnosed. ons.gov.uk — cancer survival in England
- Hopstaken JS et al. An Updated Systematic Review on Focal Therapy in Localized Prostate Cancer. European Urology. 2022;81(1):5-33.
- FTC erectile function audit (n=265). Methodology summary available on request from The Focal Therapy Clinic clinical team.
Medically authored by Dr Aqua Asif (Clinical Research Fellow, UCL Division of Surgery and Interventional Sciences) and clinically reviewed by Mr Alan Doherty (Consultant Urological Surgeon, GMC 3279241; The Focal Therapy Clinic).
Subscribe to our newsletter
Get expert advice & the latest prostate cancer research - straight to your inbox.
