
Key Takeaways
- What it does – Finasteride blocks 5-alpha reductase, lowering DHT used for an enlarged prostate (5 mg) and male pattern hair loss (1 mg).
- Prevention evidence – In the PCPT trial (~18,882 men), prostate cancer diagnosis fell ~25%, mostly low grade.
- High-grade concern – Early signal of more high-grade cancers later attributed largely to improved detection in smaller prostates.
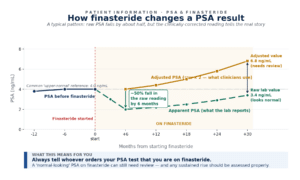
- PSA effect – Finasteride lowers PSA approximately 50%; clinicians typically interpret results by roughly doubling the value.
- What you should do – Tell every clinician you take it; a sustained PSA rise on finasteride should always be reviewed.
Finasteride lowers overall prostate cancer diagnosis by about 25% in trial settings, but mostly in lower-grade disease, and it is not used as a standard prevention or treatment medicine in Europe. Long-term follow-up has not shown higher prostate cancer mortality. Because finasteride reduces PSA by around 50%, results need careful clinical interpretation: a rising PSA still matters.

What is Finasteride
Finasteride blocks an enzyme called 5-alpha reductase. This reduces DHT, which is a hormone that helps prostate tissue grow. In practical terms, that is why finasteride can shrink an enlarged prostate over time, and why it has also been used for male pattern hair loss.
For urinary symptoms caused by benign prostatic hyperplasia, or BPH, finasteride is not a quick fix. The NHS notes that it can take up to six months to work fully. Like other medicines, it can also cause side effects, including reduced sex drive and erection problems in some men.

Why it was studied and what the trials found
As finasteride lowers DHT, which can make the prostate grow, researchers wanted to know whether finasteride might also lower the chance of prostate cancer being found.
The biggest study was the Prostate Cancer Prevention Trial, or PCPT. It included nearly 19,000 men and compared finasteride 5 mg once a day with a dummy tablet over seven years. Prostate cancer was found less often in men taking finasteride, by about 25% compared with the dummy tablet group.
That sounds impressive, but the detail matters. Most of the reduction was in lower-grade prostate cancers, which are often slower-growing. Finasteride did not become a standard medicine for preventing prostate cancer in Europe.
The original study also found more higher-grade cancers in men taking finasteride. This caused concern at the time. Later research suggested this may have been partly because finasteride shrinks the prostate, making biopsies more likely to find cancers that were already there.
Does finasteride increase the risk of high-grade prostate cancer?
The original PCPT report also showed more high-grade cancers on biopsy in the finasteride group. That finding caused understandable concern and is the main reason many men still ask, “can finasteride cause prostate cancer?”
Later analyses made the picture less alarming. Finasteride shrinks the prostate, and a smaller gland can make biopsy sampling more likely to find an existing aggressive cancer. Pathology reviews and modelling studies suggested that improved detection, and not necessarily a true cancer-causing effect, may explain much of the apparent excess of high-grade disease.
Long-term follow-up has been reassuring. In later PCPT analyses, and in a 2023 systematic review and meta-analysis of 5-alpha reductase inhibitors, use of these drugs was not associated with higher prostate cancer mortality. So, current evidence does not show that finasteride directly causes prostate cancer, but the topic still deserves careful, individual discussion.
How finasteride affects PSA testing
Finasteride can change how a PSA result looks. In men taking finasteride 5 mg for six months or more, PSA typically falls by about 50%. Even the 1 mg dose used for hair loss can lower PSA enough to matter.
That is why clinicians usually interpret PSA differently in men taking finasteride, often by roughly doubling the result once treatment has been established. This is not something patients should try to sort out themselves, because timing, trends, symptoms, and the reason for testing all matter as well.
The practical message is simple. A PSA result that looks “normal” on finasteride can still need review, and any sustained rise while taking finasteride should be assessed properly. Always tell the person ordering the test that you are taking it.
Get Expert Advice & The Latest Research
Subscribe to our newsletter to receive the latest updates, expert insights, and breakthrough research on prostate cancer-delivered straight to your inbox.
What does this mean for patients?
If you take finasteride, do not assume it protects you from prostate cancer, and do not assume it treats a cancer that is already there. The prevention data mainly relate to fewer low-grade diagnoses in a trial setting, and European guidance does not support 5-alpha reductase inhibitors as routine prevention treatment.
This point matters even more if you take finasteride for hair loss. The prevention trial used 5 mg daily, not the 1 mg dose used for male pattern hair loss, so the same prevention effect cannot be assumed.
If you already have a prostate cancer diagnosis, finasteride is not a substitute for proper specialist advice. If you are unsure what to ask next, it can help to ask a urologist why you were prescribed finasteride, what dose you are taking, and how your PSA is being interpreted.
When should you seek medical advice?
Seek medical advice if your PSA is rising while you are taking finasteride, or if you develop new or changing symptoms of prostate cancer. Prostate cancer often has no symptoms at first, and urinary symptoms can also be caused by an enlarged prostate.
Speak with a GP or specialist if you notice:
- a PSA result that is rising, or suddenly becoming harder to interpret, while on finasteride
- trouble peeing that is new, getting worse, or does not feel normal for you
- blood in your urine or semen
- ongoing back or bone pain, or unexplained weight loss
- uncertainty about why you are taking finasteride, or what dose you are on

How Focal Therapy Clinic can help
If you already have a prostate cancer diagnosis and want a clearer view of your options, the Focal Therapy Clinic’s consultants include urology, uro-radiology and oncology specialists, and cases are discussed in MDTs when considering whether focal therapy might be appropriate. Every case is reviewed carefully to match treatment to the patient.
The clinic offers minimally invasive focal treatments such as HIFU and NanoKnife. These approaches aim to treat only the cancerous area while preserving healthy prostate tissue. This can reduce the risk of incontinence and erectile dysfunction in suitable patients, compared to whole-gland treatments.
FAQs
References
European Association of Urology. (2026). EAU Guidelines on Prostate Cancer. Available at: https://uroweb.org/guidelines/prostate-cancer
NHS. (2023). About finasteride. Available at: https://www.nhs.uk/medicines/finasteride/about-finasteride/
National Cancer Institute. (2023). Prostate Cancer Prevention Trial (PCPT): Questions and Answers. Available at: https://www.cancer.gov/types/prostate/research/prostate-cancer-prevention-trial-qa
National Cancer Institute. (2019). Prostate Cancer Prevention and Finasteride: A Conversation with NCI’s Dr. Howard Parnes. Available at: https://www.cancer.gov/news-events/cancer-currents-blog/2019/prostate-cancer-prevention-finasteride-parnes
Thompson, I.M., Goodman, P.J., Tangen, C.M., et al. (2003). The influence of finasteride on the development of prostate cancer. New England Journal of Medicine, 349(3), 215-224.
Lucia, M.S., Epstein, J.I., Goodman, P.J., et al. (2007). Finasteride and high-grade prostate cancer in the Prostate Cancer Prevention Trial. Journal of the National Cancer Institute, 19(99), 1375-1383.
Cohen, Y.C., Liu, K.S., Heyden, H.L., et al. (2007). Detection bias due to the effect of finasteride on prostate volume: a modeling approach for analysis of the Prostate Cancer Prevention Trial. Journal of the National Cancer Institute, 19(99), 1366-1374.
Thompson, I.M. Jr, Goodman, P.J., Tangen, C.M., et al. (2013). Long-term survival of participants in the Prostate Cancer Prevention Trial. New England Journal of Medicine, 369(7), 603-610.
Goodman, P.J., Tangen, C.M., Darke, A.K., et al. (2019). Long-Term Effects of Finasteride on Prostate Cancer Mortality. New England Journal of Medicine, 380(4), 393-394.
Baboudjian, M., Gondran-Tellier, B., Dariane, C., et al. (2023). Association Between 5α-Reductase Inhibitors and Prostate Cancer Mortality: A Systematic Review and Meta-analysis. JAMA Oncology, 9(6), 847-850.




