
Reading Time: 5 minutes
Medically reviewed on: Aug 3th 2025 Dr Aqua Asif
Author: Neil Patel
Localised prostate cancer means the cancer is present only within the prostate and has not spread beyond it. One in eight men in the UK will be diagnosed with prostate cancer during their lifetime. For many, the diagnosis is made early, when the cancer is still localised and confined to the prostate gland. Early detection gives men more treatment choices and often leads to better outcomes.
Below we’ll explain what localised prostate cancer is, highlight its symptoms, how it is diagnosed, and the treatment options available, including why focal therapy may be the right choice for many men. If you or someone close to you has been diagnosed, knowing your options can help you make informed decisions and protect your quality of life.
Key takeaways
- Localised prostate cancer is confined to the prostate and often causes no symptoms.
- Early detection through PSA tests and MRI scans offers more treatment options.
- We use the Cambridge Prognostic Group (CPG) system in the UK, which combines PSA level, Gleason score, and cancer stages to determine the risk of progression.
- Active surveillance, focal therapy (like HIFU), surgery, and radiation are key treatment options.
- The Focal Therapy Clinic specialises in minimally invasive treatments with expert clinician-led care.
What does ‘localised’ prostate cancer mean?
Localised prostate cancer is cancer that is contained entirely within the prostate gland. In technical terms, this corresponds to clinical stages T1 or T2. It means that on detailed imaging, there is no evidence the cancer has breached the capsule (the outer layer) of the prostate or spread elsewhere.
Discovering that the cancer is localised is positive news. It means there is a very high chance of long-term control and cure. It also means that a full range of management options, from monitoring to targeted, minimally invasive treatments, are potentially available.
Are there any symptoms of localised prostate cancer?
One of the most important facts about localised prostate cancer is that it usually causes no symptoms at all. The slow growth of the tumour means it does not typically cause the urinary problems associated with a benignly enlarged prostate until much later, if ever.
The early symptoms that some men experience, such as a weaker stream or needing to urinate more frequently, are most often caused by benign prostatic hyperplasia (BPH), a non-cancerous enlargement of the gland. However, because these symptoms can overlap, it is vital to have them investigated by a doctor. The absence of symptoms is why proactive testing with a PSA blood test is so important for men who are at risk.
How is localised prostate cancer diagnosed?
A diagnosis of localised prostate cancer follows a precise, multi-step pathway designed to be as accurate as possible. The journey often begins with a PSA blood test and previously, a digital rectal examination (DRE). If either of these are abnormal, further investigation is warranted. The next and most critical imaging step is an mpMRI. This detailed scan of the prostate is excellent at identifying suspicious areas that are likely to be clinically significant cancer.
If the MRI shows a suspicious lesion, a biopsy is performed to get a definitive diagnosis. The biopsy tissue is examined by a pathologist to confirm the presence of cancer and determine its aggressiveness, which is reported as a Gleason score and Grade Group.
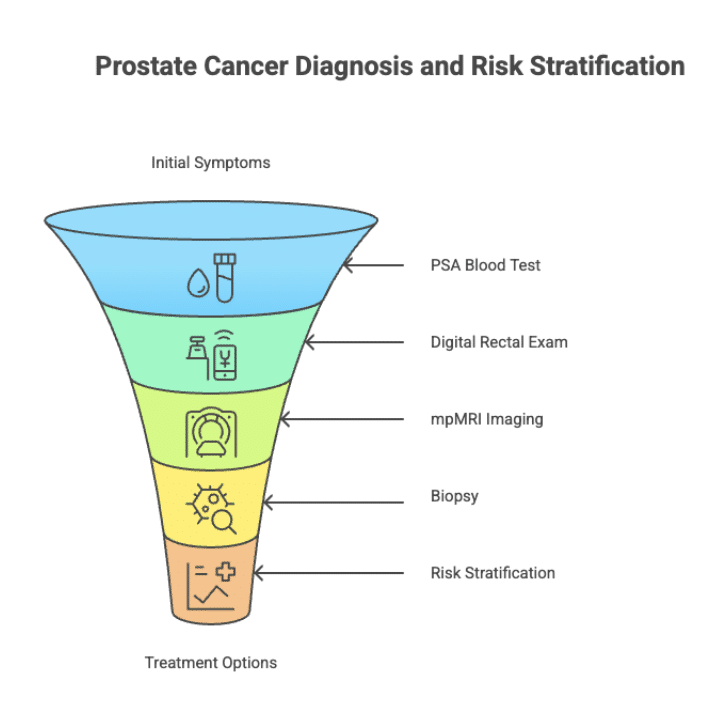
Risk categories: from low to high risk
Once cancer is confirmed, the most important step is risk stratification. We need to know how likely the cancer is to grow and cause problems. In the UK, our expert clinicians use the Cambridge Prognostic Group (CPG) system, which combines the three key pieces of information into one of five groups (CPG 1 to 5):
- PSA level: The level of prostate-specific antigen in your blood.
- Grade Group / Gleason Score: A measure of the cancer’s aggressiveness under the microscope. A Gleason score of 6 (Grade Group 1) is considered low grade. A score of 7 (Grade Group 2-3) is intermediate grade.
- T Stage: The size and extent of the tumour within the prostate.
CPG 1 is considered low-risk, while CPG 2 and 3 are intermediate-risk. CPG 4 and 5 are high-risk localised cancers. This grouping is important as it informs which treatment options are most appropriate.
Treatment options for localised prostate cancer
Choosing a treatment is a shared decision between you and your clinical team, based on your risk category, health, and personal priorities.
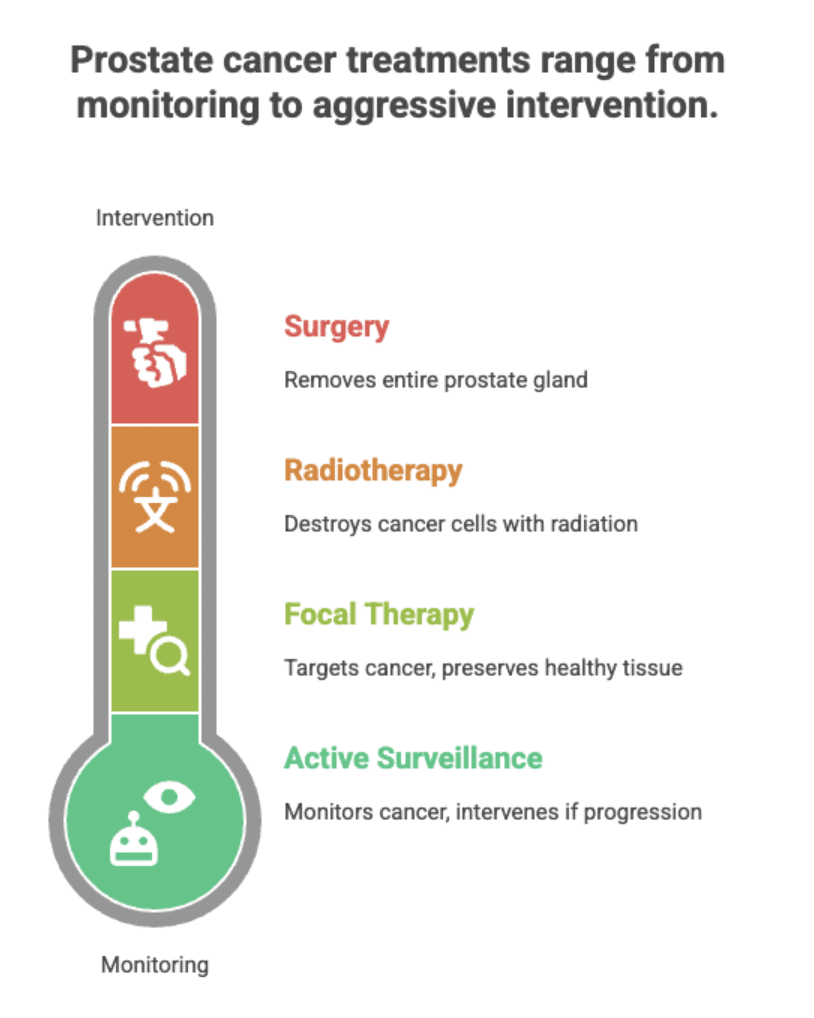
- Active Surveillance: This is the recommended international standard for men with low-risk (CPG 1) cancer. It involves monitoring the cancer with regular PSA tests and MRI scans, with the option to intervene with treatment if the cancer shows signs of progressing. The landmark ProtecT trial showed that after 15 years, survival rates were identical for men on active monitoring compared to those who had immediate surgery or radiotherapy.
- Focal Therapy: An ideal option for many men with intermediate-risk (CPG 2-3) cancer. Focal therapies like HIFU (High-Intensity Focused Ultrasound) aim to target only the cancerous part of the prostate, preserving the healthy tissue. This significantly reduces the risk of side effects like incontinence and erectile dysfunction that are more common with whole-gland treatments.
- Surgery (Radical Prostatectomy): The surgical removal of the entire prostate gland. This is an effective cancer treatment but carries a higher risk of impacting urinary control and sexual function.
- Radiotherapy: Using high-energy radiation beams to destroy the cancer cells in the whole prostate. Like surgery, it is effective but can cause side effects including bowel problems, urinary issues, and erectile dysfunction.
Get Expert Advice & The Latest Research
Subscribe to our newsletter to receive the latest updates, expert insights, and breakthrough research on prostate cancer-delivered straight to your inbox.
Why focal therapy may be the right choice
By aiming to target only the cancerous areas of the prostate, focal therapy effectively treats the disease while reducing the risk of side effects. This approach helps preserve vital functions like urinary continence and sexual health.
The Focal Therapy Clinic provides advanced focal therapy treatments, including HIFU and NanoKnife. With over 2,000 patients treated and more than 75 years of combined experience, their expert clinicians use cutting-edge imaging like PSMA scans for precise planning. They are also the only clinic using MRI-US fusion technology, further enhancing treatment accuracy.
Focal therapy is a strong option for men who meet certain eligibility criteria, such as those with low or intermediate-risk prostate cancer. The treatment is minimally invasive, with quicker recovery times compared to surgery or radiation. The clinic’s commitment to affordability for self-pay patients, combined with excellent outcomes, including a 90% success rate at one year, makes focal therapy a highly attractive choice.
What does monitoring and follow-up look like?
Whichever path is chosen, long-term monitoring is essential. After treatment, follow-up consists of regular PSA blood tests to ensure the cancer is controlled. Follow-up MRI scans are also performed periodically to check the treated area and the rest of the prostate. This structured follow-up ensures that if there is any recurrence, it is detected at the earliest possible stage when it is still easily manageable.
Conclusion
Localised prostate cancer does not always require drastic treatment or lead to life-changing side effects. By understanding what is localised prostate cancer and considering options like focal therapy, men can take control of their treatment journey. With expert clinicians providing guidance and support, patients can move forward with greater confidence and peace of mind.
FAQs
What does “localised prostate cancer” mean?
Localised prostate cancer means the cancer is contained entirely within the prostate gland. It has not spread to nearby tissues, lymph nodes, or other organs. This early stage of cancer often allows for more targeted and less invasive treatment options.
Are there symptoms of localised prostate cancer?
Most men with localised prostate cancer do not experience any symptoms. When symptoms do occur, they may include changes in urination such as increased frequency, difficulty starting, or weak flow. These symptoms are not specific to cancer and can also be caused by benign conditions like an enlarged prostate.
How is localised prostate cancer diagnosed?
Diagnosis often begins with a PSA blood test, which may be followed by an MRI scan if levels are elevated. If suspicious areas are found, a biopsy, often guided by TRUS or MRI, is used to confirm the presence of cancer. These tools help doctors understand the location, size, and aggressiveness of the tumour.
What are the treatment options for localised prostate cancer?
Treatment options include active surveillance, focal therapy (such as HIFU or cryotherapy), surgery, and radiation therapy. The best approach depends on cancer risk level, overall health, and personal preferences. Focal therapy is a popular option for preserving quality of life while effectively treating the cancer.
What risk categories exist in localised prostate cancer?
Localised prostate cancer is usually classified into low or intermediate risk based on PSA levels, Gleason score, and tumour stage. Low-risk cancers tend to grow slowly and may be managed with active surveillance. Intermediate-risk cancers may require more active treatment such as focal therapy or surgery.
References
Fendler WP, Eiber M, Beheshti M, et al. PSMA PET/CT: joint EANM procedure guideline/SNMMI procedure standard for prostate cancer imaging 2.0. Eur J Nucl Med Mol Imaging. 2023;50(5):1466-1486. doi:10.1007/s00259-022-06089-w
Macmillan Cancer Support. Prostate cancer treatment. Macmillan Cancer Support, n.d., https://www.macmillan.org.uk/cancer-information-and-support/prostate-cancer/prostate-cancer-treatment
Hamdy FC, Donovan JL, Lane JA, et al. Fifteen-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Prostate Cancer. N Engl J Med. 2023;388(17):1547-1558. doi:10.1056/NEJMoa2214122
National Institute for Health and Care Excellence (NICE). “Prostate Cancer: Diagnosis and Management.” NICE Guideline [NG131], 2019, updated 2021. www.nice.org.uk/guidance/ng131.
Cornford P, van den Bergh RCN, Briers E, et al. EAU-EANM-ESTRO-ESUR-ISUP-SIOG Guidelines on Prostate Cancer-2024 Update. Part I: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur Urol. 2024;86(2):148-163. doi:10.1016/j.eururo.2024.03.027
Gnanapragasam VJ, Bratt O, Muir K, et al. The Cambridge Prognostic Groups for improved prediction of disease mortality at diagnosis in primary non-metastatic prostate cancer: a validation study. BMC Med. 2018;16(1):31. Published 2018 Feb 28. doi:10.1186/s12916-018-1019-5
Kasivisvanathan V, Rannikko AS, Borghi M, et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N Engl J Med. 2018;378(19):1767-1777. doi:10.1056/NEJMoa1801993 Prostate Cancer UK. Localised Prostate Cancer. Prostate Cancer UK, 2023, https://prostatecanceruk.org/prostate-information-and-support/just-diagnosed/localised-prostate-cancer




